
This is a surgical procedure to bypass part of the intestine to allow malabsorption to occur.
There are 2 main procedures to consider
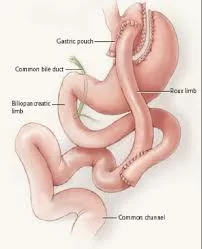
- Roux en Y Gastric bypass
- Mini gastric bypass – omega loop – single anastomosis.
These procedures encompasses a restrictive element as the stomach is reduced in volume by creating a small pouch.
The gastric bypass is classified as a restrictive and malabsorptive surgery. The Roux-en-Y Gastric Bypass is the current “gold standard” weight reduction surgery. It is the operation in which all other bariatric surgeries are compared.
The surgery is performed laparoscopically wherein the upper part of the stomach is stapled-off to create a small gastric pouch. A portion of the small bowel, the jejunum, is divided and attached to the small stomach pouch. The other small bowel end is joined back to the small bowel. With this re-routing, the remainder of the stomach and the top end of the small intestine (duodenum) are bypassed.
This operation has higher long-term rate of Type 2 Diabetes remission than restrictive procedures. A recent meta-analysis study reported an overall remission rate of 78% among diabetic patients undergoing bariatric surgery.

Advantages and disadvantages of gastric bypass surgery
Advantages:
- Minimally Invasive Surgery- small incisions, less pain, early ambulation and return to work.
- Very good for rapid remission and long term control of Type 2 Diabetes.
- Long track record.
- Usual weight loss- 60-70% of excess weight in 1-2 years.
Disadvantages:
-
bleeding – may need further surgery to stop this.
-
potentially 2 joins (anastomoses) which may leak – may require further surgery
-
internal hernias which lead to bowel obstruction/abdominal pains – which may require further surgery
-
stomach/bowel join narrowing – anastomotic strictures – may require endoscopic dilatation.
-
dumping syndrome – diarrhoea, nausea and vomiting
-
gallstones – may require gallbladder surgery.
-
stomach ulcers/perforation – may require further surgery; – high risk for patients who smoke.
-
long term – weight regain
Indications
- obesity
- failed weight loss/reflux with gastric sleeve surgery
- diabetes/metabolic health issues
- Risks
- leaks – from the anastomosis
- internal hernias/bowel obstruction
- bile reflux
Postoperative Care:
How should you prepare for the procedure?
- Discuss the operation with your close friends and family.
- Meet other patients
- Make healthier changes to your lifestyle
- Two weeks before the operation you will be required to follow a low calorie liquid diet. This will help shrink the liver and make the operation easier for the surgeon and safer for you.
The day of the operation
You will usually be admitted to the hospital on the day of your operation. You must not have anything to eat or drink (this includes chewing gum and calorie free mints) from 8 hours before your surgery, although you may drink plain water up until 2 hours before. You will then go to theatres where the anaesthetist puts you to sleep. You will also be given an intravenous drip so you can have fluids during the operation.
What should you expect after the procedure?
The day after the operation
If you have been looked after in Intensive Care you will be transferred to the ward.
The amount you may drink will be increased every couple of hours until you are able to take at least one glass of water every hour. Your drip will be removed when you are drinking enough to keep you hydrated.
The following one-two days after the operation
You should start to feel better very quickly after the operation and will be able to move around on your own.
You need to drink one 125ml glass of smooth fluid every hour when you are awake. For example you may have tea and coffee, milky drinks and soup with no lumps.
Two to three days after surgery you will be able to go home.
At discharge
Pain and medication
Sleeve gastrectomy is usually not a painful procedure. You will be given a supply of soluble painkillers to take home with you; these should be taken regularly for the first few days. If you have no pain gradually reduce the number of tablets you are taking. Allow soluble tablets to stop fizzing before you drink them. You will also prescribed an anti-acid sublingual tablet (lansoprazole fastab) to be taken daily for at least three months after your surgery.
If you have been taking medication to control your blood pressure or diabetes, these will be reviewed before your discharge. In most cases these can be reduced or sometimes stopped all together. Please make sure you are clear about this before you leave the hospital.
Please note: Do not take any large tablets for first two weeks as they may get stuck and damage the staple line. All tablets have to be crushed or taken in soluble form. If in doubt please ask your surgeon
Wounds
The small incisions made for your surgery will be more or less healed by the time you leave hospital. The steri-strips (paper stitches) should be left to come off by themselves. Any stitches will be soluble. You will only need to go home with dressings if one of the wounds is oozing. If this is the case the ward nurse will ask you to visit the nurse at your GP surgery. If any concerns, please remember that you can always refer to your surgeon
Anti-embolic stockings
You should take these home with you and continue to wear them until you are walking about on a regular basis. If you flying within six weeks from surgery, you should wear them during the flight.
Eating and Drinking
You will be given a diet information sheet. You should have this with you at all times so you know what to drink and are familiar with the stages of food introduction in the next few weeks. In case of doubt you are advised to contact your dietitian.
Washing
You can have a shower but do not soak in the bath for at least a week after surgery.
Driving
You may drive as soon as you can comfortably wear a seat belt and are able to perform an emergency stop (independently assessed by a close relative or a friend). You should check with your insurance company for their specific advice about driving after keyhole (laparoscopic) surgery.
Other Activities
You will be able to walk straight after surgery. Try to go for a walk every day, gradually increasing the distance as you feel able. You will probably need at least 2 weeks off work but please check with your surgeon. It is advisable to avoid heavy lifting for at least 1 month after abdominal surgery, if you are unsure discuss with your surgeon. You may resume sexual activity as soon as you feel comfortable.
Women of childbearing age must not become pregnant for at least one year following sleeve gastrectomy surgery. After one year: if you are planning a pregnancy please contact your dietitians for nutritional advice.
Downloads
| File | Description | File size |
|---|---|---|
 gastric-sleeve
gastric-sleeve
|
30 KB | |
|
liquid-diet
|
18 KB |

